 articles
articles
.jpg?timestamp=1480178865565)
.jpg?timestamp=1480178922275)
HOMOEOPATHIC TREATMENT OF ALZHEIMER’S DISEASE
AUTHOR: SIR DR. SINCHAN DAS
Definition of Alzheimer's disease:
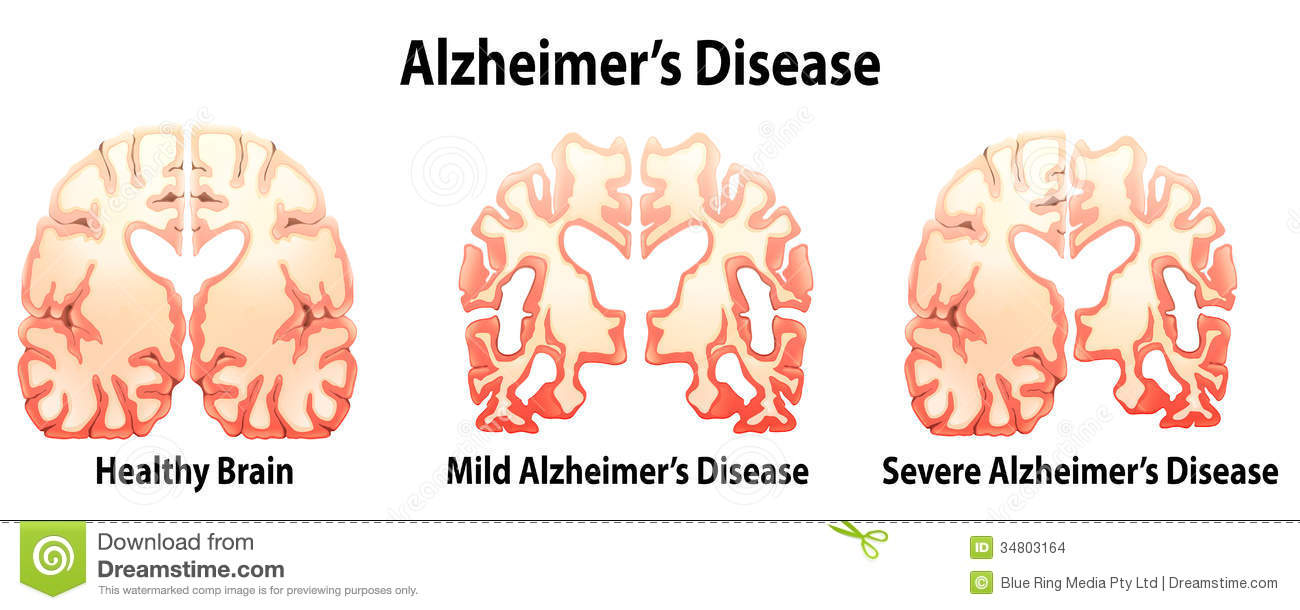
- Alzheimer's disease is a progressive, degenerative disorder that attacks the brain's nerve cells, or neurons, resulting in loss of memory, thinking and language skills, and behavioral changes.
- These neurons, which produce the brain chemical, or neurotransmitter, acetylcholine, break connections with other nerve cells and ultimately die. For example, short-term memory fails when Alzheimer's disease first destroys nerve cells in the hippocampus, and language skills and judgment decline when neurons die in the cerebral cortex.
- Two types of abnormal lesions clog the brains of individuals with Alzheimer's disease: Beta-amyloid plaques—sticky clumps of protein fragments and cellular material that form outside and around neurons; and neurofibrillary tangles—insoluble twisted fibers composed largely of the protein tau that build up inside nerve cells. Although these structures are hallmarks of the disease, scientists are unclear whether they cause it or a byproduct of it.
- Alzheimer's disease is the most common cause of dementia, or loss of intellectual function, among people aged 65 and older.
- Alzheimer's disease is not a normal part of aging.
- Origin of the term Alzheimer's disease dates back to 1906 when Dr. Alois Alzheimer, a German physician, presented a case history before a medical meeting of a 51-year-old woman who suffered from a rare brain disorder. A brain autopsy identified the plaques and tangles that today characterize Alzheimer's disease.
Origin:
Causes:
Sign and Symptoms:
Early (Mild) Stage of Alzheimers Disease
In this stage, people may:
- Forget words or misplace objects
- Forget something they just read
- Ask the same question over and over
- Have increasing trouble making plans or organizing
- Not remember names when meeting new people
Middle (Moderate) Stage of Alzheimer's Disease
In this stage, people may have:
- Increased memory loss and confusion
- Problems recognizing family and friends
- Continuously repeating stories, favorite wants
(e.g., foods, places, songs, etc.), or motions - Decreased ability to perform complex tasks
(e.g., planning dinner) or handle personal finances
(e.g., paying bills) - Lack of concern for hygiene and appearance
- Requiring assistance in choosing proper clothing
to wear for day, season, or occasion
Late (Severe) Stage of Alzheimer's Disease
In this stage, there is almost total memory loss. The individual may:
- Recognize faces but forget names
- Mistake a person for someone else
- Delusions—such as thinking he/she needs to go to work — may set in,
even though he/she no longer has a job - There is a strong need for holding something close for tactile stimulation, nurturing, companionship and comfort
- Basic abilities such as eating, walking, and sitting up fade during this period; the individual may no longer recognize when he is thirsty or hungry and will need help with all basic activities of daily living.
We know that, Alzheimer’s disease is a neurodegenerative disorder which results from many causes among which Deficiency of Sulphur is one of the causes, because Sulphur helps to maintain the cellular integrity and reactivity. But deficiency of sulphur results from many causes, among which Exposure to mercury is one of the cause. We know from our Homoeopathic concept that, functional disturbance is due to the miasm Psora; where as structural destruction is due to the syphilitic miasm. I have found 9 patients of Alzheimer’s disease till now, who are taking other mode of treatments for more than 4 years. Among those patients I have achieve success in 6 cases with only antipsoric treatment, mainly by the SULPHUR (in 50 millicimal potency).
I will discuss anther successful case of Alzheimer’s disease.
A 67 years old male patient, from Kestopur, suffering from Alzheimer’s disease from last 7 years, along with Hypertension, and BHP. He is complaining of rather better to say his family members complaining of Forgetfulness, violent anger causes throwing things, childish behavior, grinding of teeth, talkative, loss of appetite, incontinence o urine, hyperacidity, bed wetting at night, Swelling with pigmentation on the left leg etc
Past history- Recurrent low grade fever at night, Eczema on back, treated by application of ointment.
Generalities- T/R- Hot patient
Appetite- Lost
Thirst- Great thirst even if foods turns to liquid better to him
Desire- Leukewarm food, Sweet, Meat, Fried things, Condiments
Intolerance- Milk and Milk products, Fat
Stool- frequent ineffectual urging, hard burning stool, Burning anus long after passing stool
Urine- flow interrupted Sweat- profuse, offensive, sticky
Sleep- Talks during sleep, restless , catnap sleep
Treatment- 23.07.2015- Sulphur 0/3 16 dosages- Old memories starts returning, patient becomes calm than before, appetite better than before
13.08.2015- Sulphur 0/4, 16 dosages, improvement continuing
06.09.2015- Sulphur 0/5, 16 dosages, patient starts to reading books, starts to mix with the world, appetite- becomes better, stool- regular
07.10.2015- progress stopped
14.10.15- Stand still
28.10.15- new symptoms starts to come- Fear of imaginary things Alternating moods Recurrent apthous ulcer Hyperacidity, flatulence, Cramp in muscles Frequent choaking during eating Kali Brom 200/ 2 dosages is prescribed and asked the patient to come after 1 month
30.11.2015- no symptoms found of previous day. And adviced him to perform morning walk, listen soft music etc
.jpg?timestamp=1480156669403)
.jpg?timestamp=1480156852500)
Scientific Evidence for Homeopathic Medicine
By Dana Ullman, MPH
(Excepted from Consumer's Guide to Homeopathy, Tarcher/Putnam)
Although the below article is excellent, it is somewhat dated (it was written in 1995!). For a more up-to-date and comprehensive review of clinical research testing homeopathic medicines, we highly recommend that you purchase a one-time download or a 2-year subscription to a special e-book written by Dana Ullman, MPH Homeopathic Family Medicine
Most people with a little experience in homeopathy have no doubt that these medicines work, though inevitably they will have some family members, friends, neighbors, and physicians who will be skeptical about it. One way to deal with these people's skepticism is to become familiar with research on the efficacy of homeopathic medicines (see also Chapter 5 for a discussion on how to respond to skeptics' remarks; sorry, not online at present). There is actually considerably more laboratory and clinical research on homeopathic medicine than most people realize. That said, it must also be recognized that more research is certainly needed, not simply to answer the questions of skeptics but to help homeopaths optimize their use of these powerful natural medicines.
Some skeptics insist that research on homeopathy is mandatory since the exceptionally small doses used do not make sense and there is no known mechanism for action for these drugs. While it is true that homeopaths presently do not know precisely how the homeopathic microdoses work, there are some compelling theories about their mechanism of action (see the discussion in Chapter 1, "The Wisdom and Wonder of Small Doses"). More important, there is compelling evidence that they do work, as this chapter will show. And although homeopaths may not understand how their medicines work, keep in mind that leading contemporary pharmacologists readily acknowledge that there are many commonly prescribed drugs today, including aspirin and certain antibiotics, whose mechanism of action remains unknown, but this gap in knowledge has yet to stop physicians from prescribing them.
Many conventional physicians express doubt about the efficacy of homeopathy, asserting that they will "believe it when they see it." It may be more appropriate for them to acknowledge that they will "see it when they will believe it." This is not meant as a criticism of conventional physicians as much as of conventional medical thinking. The biomedical paradigm has narrowed the view of, the thinking about, and the practice of medicine to the treatment of specific disease entities with supposedly symptom-specific drugs and procedures. An integral aspect of this approach to medicine is the assumption that the larger the dose of a drug, the stronger will be its effects. While this seems to make sense on the surface, knowledgeable physicians and pharmacologists know that it isn't true. There is a recognized principle in pharmacology called the "biphasic response of drugs."1 Rather than a drug simply having increased effects as its dose becomes larger, research has consisently shown that exceedingly small doses of a substance will have the opposite effects of large doses.
The two phases of a drug's action (thus the name "biphasic") are dose-dependent. For instance, it is widely recognized that normal medical doses of atropine block the parasympathetic nerves, causing mucous membranes to dry up, while exceedingly small doses of atropine cause increased secretions to mucous membranes.
This pharmacological principle was concurrently discovered in the 1870s by two separate researchers, Hugo Schulz, a conventional scientist, and Rudolf Arndt, a psychiatrist and homeopath. Initially called the Arndt-Schulz law, this principle is still widely recognized, as witnessed by the fact that it is commonly listed in medical dictionaries under the definition of "law."
More specifically, these reseachers discovered that weak stimuli accelerate physiological activity, medium stimuli inhibit physiological activity, and strong stimuli halt physiological activity. For example, very weak concentations of iodine, bromine, mercuric chloride, and arsenious acid will stimulate yeast growth, medium doses of these substances will inhibit yeast growth, and large doses will kill the yeast.
In the 1920s, conventional scientists who tested and verified this biphasic response termed the phenomenon "hormesis," and dozens of studies were published in a wide variety of fields to confirm this biological principle.2
In the past two decades there has again been a resurgence of interest in this pharmacological law, and now hundreds of studies in numerous areas of scientific investigation have verified it.3 Because these studies have been performed by conventional scientists who are typically unfamiliar with homeopathic medicine, they have not tested or even considered testing the ultra-high dilutions commonly used in homeopathy. However, their research has consistently shown very significant effects from such small microdoses that even the researchers express confusion and surprise.
Reference to this research on the Arndt-Schulz law and hormesis is important for validating homeopathic research because it demonstrates the evidence for the important biphasic responses and microdose effects that lie at the heart of homeopathy. This research is readily available to physicians and scientists yet is often ignored or not understood.
The amount of research on homeopathic medicines is growing, and it is becoming increasingly difficult to ignore these studies, because they are now appearing in many of the most respected medical and scientific journals in the world. This chapter is not meant to be exhaustive (that would require a book or two of its own). It will include many of the best studies, most of which have been published in conventional medical and scientific journals. Some of the studies are discussed because of the impressive results they showed, and others are included for their implications for better understanding homeopathy and the healing process. The review of research is not simply to provide evidence of the efficacy of homeopathic medicine but also to enlighten readers on how to evaluate homeopathic research, whether positive or negative results are obtained.
To best understand the remaining part of this chapter, some definitions are helpful:
--Double-blind trials refer to experiments in which neither the experimenter nor the subjects know whether a specific treatment was prescribe or a placebo (a fake medicine that looks and tastes like real homeopathic medicines).
--Randomized trials are those in which subjects of an experiment are randomly placed either in treatment groups or in placebo groups. The researchers attempt to place people with similar characteristics in equal numbers in treatment and placebo groups.
--Crossover studies refer to experiments in which half of the subjects of a study are given a placebo during one phase of a study and then given the active treatment during the second phase, while the other half begin with the active treatment and then receive the placebo during the second phase. Crossover studies sometimes do not test a placebo and instead compare one type of treatment with another type of treatment.
Modern research is designed to evaluate the results of a therapy as compared to a placebo and/or another therapy. This type of study is valuable because many patients respond very well to placebos, and this "treatment" is so safe and inexpensive it is generally assumed that "real treatments" should have considerably better results than placebo medicine. One should note that placebo effects can be significant, and clinically, these effects can be very positive (some people think of them as a type of self-healing).
Double-blinding an experiment is important to research because experimenters tend to treat people who are getting the real treatment differently or better than those given a placebo, thus throwing off the results of the experiment. Research is randomized so that those people treated with the real medicine and those treated with the placebo are as similar as possible, making a comparison between real treatment and placebo treatment more accurate. Crossover studies allow researchers to compare the separate effects of a placebo and a treatment on all subjects in an experiment.
Statistics obviously are an important part of research. A treatment is thought to be considered better than a placebo if the results, according to statistical analysis, have no more than a 5% possibility of happening at random (the notation of this statistical probability is: P=.05). A study with a small number of patients (for example, 30 or less) must show a large difference between treatment and nontreatment groups for it to become statistically significant. A study with a large number of patients (for example, several hundred) needs to have only a small but consistent difference to obtain a similar statistical significance. This information is provided so that readers will know that all the studies described in this chapter are statistically significant, except when otherwise noted.
Clinical Research
People are often confused by research, not only because it can be overly technical but because some studies show that a therapy works and other studies shows that it doesn't. To solve this problem, a recent development in research is used, called a "meta-analysis," which is a systematic review of a body of research that evaluates the overall results of experiments.
In 1991, three professors of medicine from the Netherlands, none of them homeopaths, performed a meta-analysis of 25 years of clinical studies using homeopathic medicines and published their results in the British Medical Journal.4 This meta-analysis covered 107 controlled trials, of which 81 showed that homeopathic medicines were effective, 24 showed they were ineffective, and 2 were inconclusive.
The professors concluded, "The amount of positive results came as a surprise to us." Specifically, they found that:
13 of 19 trials showed successful treatment of respiratory infections,
6 of 7 trials showed positive results in treating other infections,
5 of 7 trials showed improvement in diseases of the digestive system,
5 of 5 showed successful treatment of hay fever,
5 of 7 showed faster recovery after abdominal surgery,
4 of 6 promoted healing in treating rheumatological disease,
18 of 20 showed benefit in addressing pain or trauma,
8 of 10 showed positive results in relieving mental or psychological problems, and
13 of 15 showed benefit from miscellaneous diagnoses.
Despite the high percentage of studies that provided evidence of success with homeopathic medicine, most of these studies were flawed in some way or another. Still, the researchers found 22 high-caliber studies, 15 of which showed that homeopathic medicines were effective. Of further interest, they found that 11 of the best 15 studies showed efficacy of these natural medicines, suggesting that the better designed and performed the studies were, the higher the likelihood that the medicines were found to be effective. Although people unfamiliar with research may be surprised to learn that most of the studies on homeopathy were flawed in one significant way or another,5 research in conventional medicine during the past 25 years has had a similar percentage of flawed studies.
With this knowledge, the researchers of the meta-analysis on homeopathy concluded, "The evidence presented in this review would probably be sufficient for establishing homeopathy as a regular treatment for certain indications."
There are different types of homeopathic clinical research, some of which provide individualization of remedies; which is the hallmark of the homeopathic methodology; some of which give a commonly prescribed remedy to all people with a similar ailment, and some of which give a combination of homeopathic medicines to people with a similar condition. While one can perform good research using any of these methods, there are certain issues that researchers have to be aware of and sensitive to in order to obtain the best objective results.
For instance, if a study does not individualize a homeopathic medicine to people suffering from a specific ailment and the results of the study show that there was no difference between those given this remedy and those given a placebo, the study does not disprove homeopathy; it simply proves that this one remedy is not effective in treating every person suffering from that ailment, each of whom may have a unique pattern of symptoms that requires an individual prescription.
In describing specifics of the following studies using homeopathic medicines, differentiation has been made between studies that allowed for individualization of medicines and those that did not.
Clinical Research with Individualized Care
Some people incorrectly assume that research using homeopathic medicines is impossibly complicated because each medicine must be individualized to the patient. The following studies disprove this simplistic belief.
A recent clinical trial evaluating homeopathic medicine was a unique study of the treatment of asthma.6 Researchers at the University of Glasgow used conventional allergy testing to discover which substances these asthma patients were most allergic to. Once this was determined, the subjects were randomized into treatment and placebo groups. Those patients chosen for treatment were given the 30c potency of the substance to which they were most allergic (the most common substance was house dust mite). The researchers called this unique method of individualizing remedies "homeopathic immunotherapy" (homeopathic medicines are usually prescribed based on the patient's idiosyncratic symptoms, not on laboratory analysis or diagnostic categories). Subjects in this experiment were evaluated by both homeopathic and conventional physicians.
This study showed that 82% of the patients given a homeopathic medicine improved, while only 38% of patients given a placebo experienced a similar degree of relief. When asked if they felt the patient received the homeopathic medicine or the placebo, both the patients and the doctors tended to guess correctly.
The experiment was relatively small, with only 24 patients. As noted, for statistically significant results, small experiments must show a large difference between those treated with a medicine and those given a placebo. Such was the case in this study.
Along with this recent asthma study, the authors performed a meta-analysis, reviewing all the data from three studies they performed on allergic conditions, which totaled 202 subjects. The researchers found a similar pattern in the three studies. Improvement began within the first week and continued through to the end of the trial four weeks later. The results of this meta-analysis were so substantial (P=0.0004) that the authors concluded that either homeopathic medicines work or controlled clinical trials do not. Because modern science is based on controlled clinical trials, it is a more likely conclusion that homeopathic medicines are effective.
Another recent study, published in the American journal Pediatrics, tested homeopathic medicine for the treatment of a condition recognized to be the most serious public health problem today, childhood diarrhea.7 Over 5 million children die each year as the result of diarrhea, mostly in nonindustrialized countries. Conventional physicians prescribe oral rehydration therapy (ORT, a salt solution that helps children maintain fluid balance), but this treatment does not fight the infection that underlies the diarrhea.
Conducted in Nicaragua in association with the University of Washington and the University of Guadalajara, this randomized double-blind, placebo-controlled study of 81 children showed that an individually chosen remedy provided statistically significant improvement of the children's diarrhea as compared to those given a placebo. Children given the homeopathic remedy were cured of their infection 20% faster than those given a placebo, and the sicke children responded most dramatically to the homeopathic treatment. A total of 18 different remedies were used in this trial, individually chosen based on each child's symptoms.
A study of the homeopathic treatment of migraine headache was conducted in Italy.8 Sixty patients were randomized and entered into a double-blind, placebo-controlled trial. Patients regularly filled out a questionnaire on the frequency, intensity, and characteristics of their head pain. They were prescribed a single dose of a 30c remedy at four separate times over two-week intervals. Eight remedies were considered, and prescribers were allowed to use any two with a patient. While only 17% of patients given a placebo experienced relief of their migraine pain, an impressive 93% of patients given an individualized homeopathic medicine experienced good results.
A randomized double-blind, placebo-controlled trial was performed on 175 Dutch children suffering from recurrent upper respiratory tract infections.9 Children in the treatment group were prescribed a "constitutional medicine" for their overall health as well as acute medicines to treat the acute respiratory infections they developed. The study found that the children given homeopathic medicines had a 16% better daily symptom score than children given a placebo.
This study also found that the number of children given a placebo who had to undergo adenoidectomy was 24% higher than for the children given homeopathic remedies. A 54.8% reduction in the use of antibiotics in the children given homeopathic medicines was reported, while the children who received a placebo experienced a 37.7% reduction in antibiotic use. (This reduction in both groups was determined to be the result of the normal growth and development of the child, dietary changes° the study provided written nutritional advice to the parents° and the change in expectations as the result of being under medical care.)
The statistical possibility of these results happening by chance was 6% (P=0.06). Because statistical significance in science is recognized when there is a 5% or less chance of results happening at random, the researchers concluded that homeopathic medicine seem to add little to the treatment of upper respiratory tract infections. This more conservative conclusion appeared to be influenced by the fact that the authors sought and received publication of their study in the British Medical Journal. They should have more accurately said that homeopathic medicines provided benefit to children with upper respiratory infections, but there is a small chance (6%) that these good results happened at random.
Considering the closeness of these results to 5%, considering the other improvements in the homeopathic group's health, and considering the increasingly widespread desire to avoid antibiotics, it makes sense for physicians and parents to consider seeking homeopathic care for children's upper respiratory infections.
Another study that involved individualized homeopathic care was in the treatment of rheumatoid arthritis.10 The study involved 46 patients. Two homeopathic physicians prescribed individually chosen medicines to each patient, though only half of them were given the real remedy, while the other half were given a placebo. The study found that 82% of those given an individualized homeopathic remedy experienced some relief of symptoms, while 21% of those given a placebo experienced a similar degree of relief.
One other very interesting trial that utilized semi-individualization of care was in the treatment of primary fibromyalgia (also called fibrositis).11 Patients with fibrositis were admitted into a trial in which homeopathic physicians chose between three possible remedies, Arnica, Rhus tox, and Bryonia. Half of the patients were given one of these remedies, and the other half were given a placebo. There was no discernible difference between these groups. However, as an integral part of the experiment's design, a panel of homeopaths evaluated the accuracy of each prescription. This analysis found that those patients whom the panel considered to have received the correct remedy experienced a statistically significant improvement in symptoms as compared to those patients given the "incorrect" remedy or the placebo.
These same researchers next conducted a more sophisticated trial in the treatment of primary fibromyalgia.12 This double-blind, placebo-controlled, crossover trial admitted only those patients who fit the symptoms of Rhus tox. The researchers found that this constituted 42% of the patients interviewed. One-half of these 30 patients were given Rhus tox 6c during the first phase of the experiment, while the other half were given a placebo. During the second phase, those patients initially given the medicine were given a placebo, and those patients initially given a placebo were now given the homeopathic remedy. Researchers determined at the beginning of the experiment that improvement in pain and sleeplessness were the outcome measures most important in evaluating the results of this trial, and the results showed that 25% more of the patients experienced pain relief when taking the homeopathic remedy compared to when they were given a placebo and almost twice as many had improved sleep when taking the remedy.
This type of crossover design is considered a sophisticated type of research because it compares each person when using a treatment with the same person when using a placebo. Most other research compares two supposedly similar groups of people, but researchers commonly acknowledge that it is difficult and perhaps impossible to get two exactly similar groups of people. The limitation of the crossover design for homeopathic treatment, however, is that most homeopathic medicines provide long-term benefits, so that once a person stops taking a homeopathic remedy he or she may still continue to improve, even in the placebo stage of the trial. Low-potency medicines, such as the 6c used in the above described experiment, generally have short-acting effects, while higher potency medicines generally have increasingly longer-term effects.
Clinical Research with Non individualized Care
In addition to the studies on homeopathy in which individualized remedies are prescribed, there is also a body of research testing single remedies to people given in a non-individualized manner. Such research is potentially problematic because homeopaths acknowledge that the remedies require some degree of individualization to be effective. The results of a nonindividualized study, either positive or negative, can be misunderstood by people who do not know basic principles of the homeopathic method.
One study using nonindividualized homeopathic treatment was sponsored by the British government during World War II and was conducted in 1941-42 on volunteers whose skin was burned with mustard gas.13 The study showed the efficacy of Mustard gas 30c as a preventive or Rhus tox 30c and Kali bichromicum 30c as therapy. The study was double-blind, placebo-controlled, and was conducted at two centers (London and Glasgow), both showing similarly positive results. A more recent analysis of the data further substantiated the statistical significance of this study.14
It should, however, be mentioned that the researchers also tested the efficacy of Opium 30c, Cantharis 30c, and Variolinium 30c, none of which provided any noticeable benefit. If this trial had tested only these medicines, the researchers might have concluded that homeopathic medicines were ineffective in treating mustard gas burns. Finding the correct remedy is the key to making homeopathy work.
Some skeptics and journalists inaccurately report that homeopathy is primarily used to treat minor health problems. Homeopaths today primarily treat various chronic ailments for which conventional medicine has not provided effective treatment. One example of a chronic and serious problem shown by a controlled study to be effective treated by homeopathy is diabetic retinitis15 (retinitis is a common complication of diabetes in which there is an inflammation of the retina causing impairment of sight, perversion of vision, swelling, discharge from the eye, and sometimes hemorrhages into the retina). This double-blind, randomized, placebo-controlled study on 60 patients used Arnica 5c. The results of this study showed that 47% of patients given Arnica 5c experienced improvement in central blood flow to the eye, while only 1% of patients given the placebo experience this improvement. Further, 52% of patients given Arnica 5c experienced improvement in blood flow to other parts of the eye, while only 1.5% of those given the placebo experienced a similar degree of improvement.
The best-selling flu remedy in France is actually a homeopathic medicine. Anas barbariae 200c, commonly marketed under the trade name Oscillococcinum TM
Oscillococcinum is also popular in the U.S. and is effective primarily at the first signs of influenza. A double-blind, placebo-controlled study with 478 patients suffering from influenza was conducted, making this the largest trial yet performed testing a homeopathic medicine.16 This trial showed that almost twice as many people who took the homeopathic remedy got over the flu after 48 hours as compared to those given a placebo.
Although this remedy was found to work for all age groups, it was considerably more effective for people under 30 than for those over 30. However, it was not found to be effective when subjects had severe flu symptoms. In severe cases of the flu, a more individualized homeopathic remedy may be indicated.
In addition to various studies on human health, there have also been some animal studies. British researchers have conducted trials showing that homeopathic medicines, specifically Caulophyllum 30c, could lower the rate of stillbirths in pigs.17 Pigs given a placebo had 103 births and 27 stillbirths (20.8%), while those given Caulophyllum 30c had 104 births and 12 stillbirths (10.3%).
Not all studies show efficacy of homeopathic medicines, not because they don't work but mostly because the studies were poorly designed. One such study tested a single homeopathic medicine in the treatment of osteoarthritis.18 This study consisted of 36 patients, of whom one third were given Rhus tox 6c, one third were given a conventional drug (fenoprofen, a nonsteroidal anti-inflammatory drug), and one third were given a placebo. Those patients given the conventional drug experienced some relief of symptoms, but those given the homeopathic remedy and the placebo had a similar lack of response to treatment. While some people would erronously conclude that homeopathic medicines are ineffective in the treatment of osteoarthritis, it would be more appropriate and accurate to conclude that Rhus tox 6c is an ineffective remedy when given without individualization to people with osteoarthritis.
One of the confounding variables from this trial was that 2 of the 12 patients given the homeopathic medicine were withdrawn from the trial because they experienced an aggravation of symptoms after taking the medicine. Because homeopathic medicines sometimes cause a temporary increase in chronic symptoms before significant improvement, it was disappointing that the researchers did not follow their status. Because this trial lasted only two weeks, it did not allow time for the homeopathic remedy to be adequately evaluated. If, for instance, these 2 patients experienced the significant relief that is common after an initial aggravation of symptoms, the results of the trial would have been different.
Further, it is unfair to compare a fast-acting conventional drug that has side effects with a slower acting homeopathic medicine that is considerably safer. Finally and of great significance is the fact that while Rhus tox is a common remedy for rheumatoid arthritis, it is less common for osteoarthritis.
Clinical Research with Homeopathic Combination Remedies
Homeopathic combination remedies are formulas in which several homeopathic substances are mixed together into one remedy. This untraditional approach to using homeopathic medicine is commercially popular in many countries. While these remedies are not thought by homeopaths to be as effective as individually chosen medicines, they do work and research has verified this. Yet, homeopaths consistently find that single homeopathic medicines have the potential to truly cure a person's disease, while combination medicines at best provide safe but temporary relief of symptoms.
The same researchers who conducted the study on asthma earlier described also performed a study on the treatment of hayfever.19 This double-blind, placebo-controlled study prescribed a 30c potency of a combination remedy made from 12 common pollens. The results showed that those subjects taking the homeopathic remedy had six times fewer symptoms than those given the placebo. Both groups of subjects were allowed to use an "escape" medicine (an antihistamine) if their remedy didn't work adequately. The study showed that homeopathic subjects needed this medicine half as often as did those given the placebo.
Another example of significant results from a homeopathic combination remedy was in the treatment of women during their ninth month of pregnancy.20 Ninety women were given the 5c potency of the following remedies: Caulophyllum, Arnica, Cimicifuga, Pulsatilla, and Gelsemium. They were given doses of this combination remedy twice daily during the ninth month. This double-blind, placebo-controlled study showed that women given the homeopathic medicines experienced a 40% (!) shorter labor than those given a placebo. Also, the women given the placebo had four times (!) as many complications of labor as those given the homeopathic medicines.
One of the limitations of research on combination remedies is that the results do not reveal whether the effective treatment came from one specific medicine or from the unique combination of remedies. A recent study of 22 healthy women in their first pregnancies tested Caulophyllum, one of the medicines used in the study cited above, which was administered in the 7c potency during the active phase of labor (one dose per hour repeated for a maximum of 4 hours). The time of labor for those women given the homeopathic medicine was 38% shorter than for women given a placebo.21 This trial was not double-blind; however, the researchers recently completed a double-blind trial and confirmed their earlier results.22
A popular homeopathic external application marketed as TraumeelTM has been studied for its efficacy in the treatment of sprained ankles.23 This combination of 14 remedies in 2x to 6x potencies was given to subjects with sprained ankles. After 10 days, 24 of the 33 patients who were given the homeopathic medicine were pain-free, while 13 of 36 patients given a placebo experienced a similar degree of relief. This same medicine was also used in the treatment of traumatic hemarthrosis (joint swelling) and was shown to significantly reduce healing time as compared to a placebo. Objective measurements of joint swelling and movement and evaluation of the synovial fluid at injury were assessed.24
A study of 61 patients with varicose veins was performed double-blind and placebo-controlled.25 Three doses of a popular German combination of eight homeopathic medicines were given daily for 24 days. Measures were venous filling time, leg volume, and subjective symptoms. The study found that venous filling time improved in those given the homeopathic medicines by 44%, while it deteriorated in the placebo group by 18%. Other measures also had significant differences.
In addition to the various clinical studies on humans, there has also been some research using homeopathic medicines to improve the health of animals. German researchers have shown that dairy cows given Sepia 200c experienced significantly fewer complications of birth than those given a placebo.26 Low-potency (1x to 6x) combinations of Lachesis, Pulsatilla, and Sabina, or Lachesis, Echinacea, and Pyrogenium, along with Caulophyllum given to pigs had preventive and therapeutic effects on infections (inflammation of the breasts and the uterus) as well as on diarrhea in the piglets.27
Not all clinical studies on homeopathic combination medicines find efficacy of treatment, but there are often important factors that explain the failure. A Canadian study on the treatment of plantar warts is one such example.28 This randomized double-blind, placebo-controlled trial with 162 patients prescribed three medicines to each patient (Because the trial did not mix the remedies together, it is not completely accurate to call the use of these remedies a combination. It is more precise to consider it "polypharmacy," the use of several medicines). The remedies used were Thuja 30c, Antimonium crud 7c and Nitric acid 7c. Thuja was taken once a week, and the other two remedies were taken once a day. The trial lasted six weeks. The results showed that there was no noticeable difference between those subjects given the homeopathic medicines and those given a placebo.
Many homeopaths may be initially surprised at the result of this trial because they consider these remedies commonly effective in the treatment of warts. But while the remedies may be effective for treating warts, they are not necessarily effective for all types of warts or in all people. A recent study of homeopathic treatment for various types of warts found that 18 of 19 people with plantar warts were cured in, on average, 2.2 months.29 The most common remedy was Ruta, prescribed to 12 of the 19 patients. Thuja was prescribed for only 3 patients, and Antimonium crud was prescribed for 2 patients.
This study teaches us that individualization and the use of well-chosen remedies are necessary for most effective treatment.
One additional note about research using homeopathic combination medicines: The homeopathic literature refers to the fact that some remedies are antidoted by other remedies. While the medicines in the Canadian trial are not known to antidote each other, homeopaths acknowledge that our understanding of which remedies antidote each other is somewhat primitive (for a listing of which remedies antidote each other, see the appendix in Kent's Repertory or in the Indian edition of Boericke's Pocket Manual of Materia Medica with Repertory). Homeopathic research must, therefore, be aware of this possibility so that conclusions from research are not overstated.
Laboratory Research
As valuable as clinical studies are, laboratory research is able to show biological activity of homeopathic medicines that cannot be explained as a placebo response, a common accusation of skeptics. Laboratory research is also capable of shedding some light on how the homeopathic medicines may work.
Distinct from clinical research which seeks to measure improvement in the health of a person or an animal, laboratory research seeks to assess changes in biological systems (cells, tissues, organs, viruses, etc.). Typically, animal research can fit under either clinical or laboratory research, depending on the goal of the study. If the study seeks to test the efficacy of a treatment on the health of an animal, it can be considered an animal clinical study. If the study seeks to test the effects of a treatment on animals so that researchers can apply the information for human health or to understand biological phenomena, it can be considered a laboratory study.
Admittedly, while some of the animal studies discussed here are humane, others are not. Reference to these studies is not meant to suggest that this author condones all such research. Rather, discussion of these studies is intended to verify the benefits of homeopathic medicines, both to animals and to humans, and to encourage wider use of homeopathic remedies.
Some of this section is somewhat technical, though an effort has been made to describe the studies in a user-friendly manner.
Earlier in this chapter, reference was made to some important double-blind clinical research with homeopathic medicines conducted as far back as 1941. There were also some high-quality scientific laboratory studies investigating homeopathic microdoses as that time. One extensive and meticulously controlled study was performed in 1941-42 by a Scottish homeopath/scientist, W.E. Boyd.30 This work showed that microdoses of mercuric chloride had statistically significant effects of diastase activity (diastase is an enzyme produced during the germination of seeds). This research was so well designed and performed that an associate dean of an American medical school commented, "The precision of [Boyd's] technique exemplifies a scientific study at its highest level."31
There have been over 100 studies evaluating the prophylactic and therapeutic effects of homeopathic doses of normally toxic substances. A collaborative effort of scientists from German research institutions and from America's Walter Reed Hospital performed a meta-analysis of these studies.32 Like the meta-analysis described earlier on clinical trials using homeopathic medicines, most of the studies were flawed in some way. However, of the high quality studies, positive results were found 50% more often than negative results. What was particularly intriguing was that researchers who tested doses in the submolecular range (potencies greater than 24x) were found to have the best designed studies and more frequently found statisticially significant results from these microdoses. Specifically, several researchers gave, usually to rats, crude doses of arsenic, bismuth, cadmium, mercury chloride, or lead. The research showed that animals who were pretreated with homeopathic doses of these substances and then given repeated homeopathic doses after exposure to the crude substance, excreted more of these toxic substances through urine, feces, and sweat than did those animals given a placebo.
Several studies noted that pretreatment and treatment with potentized doses of substances different from those to which the animal was being exposed did not provide any benefit.
As horrible as this research may be for the animals tested, animal researchers claim that it can have considerable benefit for treating animals and humans exposed to toxic substances. Such studies cannot be performed humanely on human subjects, and because of the newness of the research, no computer models to simulate the effects of homeopathic medicines are presently possible. While public health measures must primarily focus on preventing exposure to toxic substances, medical treatment must be developed for healing if and when exposure takes place. The research suggests that homeopathic medicine may play a significant role in the treatment of toxicological exposure.
Homeopathic research has also explored the benefits of homeopathic medicines to protect against radiation.33 Albino mice were exposed to 100 to 200 rad of X-rays (sublethal doses) and then evaluated after 24, 48, and 72 hours. Ginseng 6x, 30x, and 200x and Ruta graveolens 30x and 200x were administered before and after exposure. When compared with mice given a placebo as treatment, mice given any of the above homeopathic medicines experienced significantly less chromosomal or cellular damage.
Albino guinea pigs were exposed to small doses of X-ray that cause reddening of the skin. Studies showed that Apis mellifica 7c or 9c had a protective effect and a roughly 50% curative effect on X-ray-induced redness of the skin.34 Apis mellifica (honeybee) is a homeopathic medicine for redness, swelling, and itching, common symptoms of bee venom.
In one very intriguing study, Thyroxine 30x (thyroid hormone) was placed in the water of tadpoles.35 When compared to tadpoles who were given a placebo, the study showed, morphogenesis of the tadpoles into frogs was slowed for those who were exposed to the homeopathic doses. Because thyroid hormone in crude doses is known to speed up morphogenesis, it makes sense from a homeopathic perspective that homeopathic doses would slow it down.
What makes this study more interesting is that additional investigations resulted in the same effect when a glass bottle of the homeopathic doses of thyroid hormone was simply suspended in the water with the lip of the bottle above the water line. This research was replicated at several laboratories, and results were consistent.
The implications of this study are somewhat significant, not only for verifying biological effects of homeopathic doses but for showing that these medicines have some type of radiational effect through glass. Some types of unconventional approaches to homeopathy have been developed over the past decades in which pupil reflex, pulse, muscle strength, and skin conductance have been changed as the result of simply holding on to a bottle of an individually indicated homeopathic medicine. While this approach may seem strange to classically oriented homeopaths, the above research provides some basis for its application.
One other interesting experiment dealing with water is worthy of mention. This study used nuclear magnetic resonance (NMR), also called magnetic resonance imaging (MRI), to determine whether high potencies of homeopathic medicines placed in water had any measurable effects.36 Without getting into the details of this highly technical study, the researchers found that high potencies of Silicea did, in fact, show a distinct difference as compared with placebo-treated water.
There have been several studies investigating very high dilutions of histamine (above 30x) on isolated guinea pig hearts, showing that this remedy increases blood flow through the heart. What is particularly interesting about these studies was that this effect was completely neutralized if the very high dilutions were exposed to 70 degrees Centigrade for 30 minutes or exposed to magnetic fields of 50 Hz for 15 minutes.37 Needless to say, it is unlikely that these microdoses could have only a placebo effect when known physical stresses to the medicine can halt its activity.
A professor of hematology at the School of Pharmacy of Bordeaux has carried out eight years of research on the effects of acetylsalicylic acid (the active ingredient in aspirin) on blood.38 It is known that crude doses of aspirin cause increased bleeding, while this research showed that homeopathic doses of acetylsalicylic acid shorten bleeding time in healthy subjects.
Two Dutch professors of molecular cell biology recently completed a significant body of experimentation which not only provided evidence of the effects of homeopathic microdoses on cell cultures but that also suggested that these microdoses are only effective when homeopathy's principle of similars is followed.39 Specific reference to the body of studies cannot be provided in this chapter, both due to the space necessary to describe this work and due to its highly technical nature.
A now famous study by respected French physician and immunologist Jacques Benveniste tested highly diluted doses of an antibody on a type of white blood cells called basophils (basophils increase in number when exposed to substances such as antibodies which cause an allergic reaction). This work was replicated at six different laboratories at four different universities (the University of Paris South, the University of Toronto, Hebrew University, and the University of Milano). Although the prestigious journal Nature published this study,40 it also published concurrently an editorial stating that they did not believe the results.41 The editor insisted on going to the primary researcher's laboratory at the University of Paris South to observe the experiment conducted in his presence along with two known experts in scientific fraud (one of whom was a magician).
The details of what followed require more detail and technical information than is appropriate for this book. In summary, the experiment did not show significant results, leading the Nature editor to pronounce in his journal that the original study was a fraud.42 The problem, however, was that the editor and the fraud experts were not immunologists, and thus, they did not seem aware that many studies in immunology require considerably more replication than could be done in the couple of days that the Nature team visited.
Another problem was in the study itself, which was very difficult to do. The researchers later simplified it, provided even greater scientific controls, and found significant results. Nature, however, chose not to publish these results, and this study was published instead in the Journal of the French Academy of Sciences.43
Evidence of the bias that "defenders of science" have against homeopathy is their refusal to publish or even comment on the increasing body of research accruing to homeopathic medicine.
Science is supposed to be objective, though both physicists and psychologists teach us that objectivity is impossible. Science's long-term antagonism to homeopathy is slowly breaking down but not without significant reaction, fear, anxiety, and sometimes downright attack against homeopaths.
Change is difficult, and significant change is even more difficult. Even though science grows from new knowledge, it tends to be resistant, often very resistant, to perspectives and knowledge that do not fit contemporary paradigms and scientific theories. The information presented in this chapter and in this book is not meant to overthrow science but to enlarge its perspective so that it more broadly and accurately describes and accepts many presently unexplainable phenomena of nature.
In Summary
This review of research is not meant to be complete. Readers are encouraged to review the books listed in the Resources section of this chapter for access to many other clinical and laboratory studies as well as to theoretical foundations of homeopathic microdoses.
Despite the now strong evidence that homeopathic medicines promote biological activity and clinical efficacy, there is still great resistance to them. Recently, the Lancet published the research on the homeopathic treatment of asthma.44 In a press release announcing this research, they emphasized that although homeopathic medicines may provide some benefit to people with asthma, conventional medicines offer greater benefit.
This was a strange statement for two reasons. First, the study didn't compare homeopathic and conventional medicine; it only compared homeopathic medicine with a placebo. Any other conjecture was not founded on the data presented. Secondly, the Lancet refused to openly acknowledge that homeopathic medicines may work after all.
One can't help but wonder whether if a man flew and science proved that he flew, the editors of some medical journals would remark: "But he doesn't fly as high or as fast as a jet plane!"
Despite the resistance to change in general and to homeopathy specifically, it is getting increasingly difficult for physicians and scientists to doubt the benefits that homeopathic medicines offer. Italian hematologist Paolo Bellavite and Italian homeopath Andrea Signorini's Homeopathy: A Frontier in Medical Science is presently the most comprehensive resource of controlled studies on homeopathy. The authors conclude, "The sum of the clinical observations and experimental findings is beginning to prove so extensive and intrinsically consistent that it is no longer possible to dodge the issue by acting as if this body of evidence simply did not exist."45
They go on to say, "To reject everything en bloc, as many are tempted to do, means throwing out the observations along with the interpretations, an operation which may be the line of least resistance, but which is not scientific because unexplained observations have always been the main hive of ideas for research."
To ignore the body of experimental data that presently exists on homeopathic medicines and to deny the body of clinical experience of homeopaths and homeopathic patients, one would have to be virtually blind. One can only assume that this blindness is a temporary affliction, one that will soon be cured.
